Emergency aid and disaster response is as old as humanity. Chaos cannot be prevented during the initial period of a major disaster, but it has to be the aim of every disaster operation plan to keep this time as short as possible.
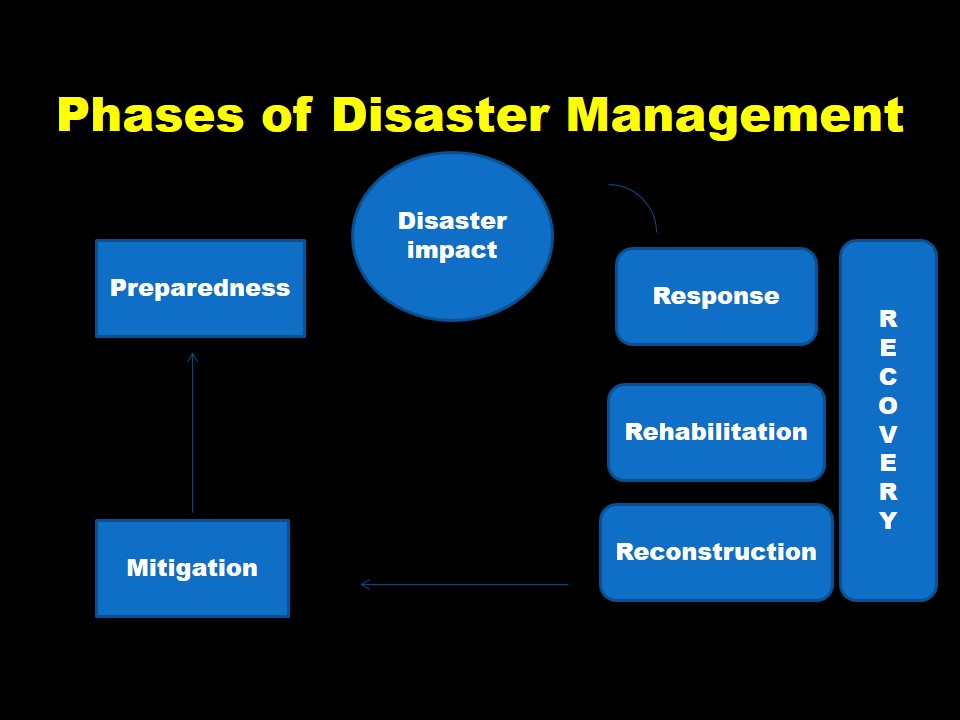
Preparedness
Planning how to respond for an emergency or disaster and working to increase resources available to respond effectively. This is a multisectorial activity and involves following departments:
- communications
- health
- social welfare
- police & security
- search & rescue
- transport
- media
Preparedness may be divided into:
• Pre-disaster Preparedness
• Post-disaster Preparedness
Efficient action has to be taken at all levels to save lives, reduce sufferings & minimize damage to property. Important tasks for preparedness include:
- evaluate risk,
- adopt standards/regulations,
- organize communication, warning systems, coordination& response mechanism,
- ensure financial resources,
- develop public education programmes,
- coordinate with media, and
- organize disaster simulation exercises
Planning Process
P Planning
O Organizing
S Staffing
D Directing
C Coordinating
R Reporting
B Budgeting
Disaster Impact & Response
Activities that occur during and immediately following a disaster. These include:
- Search, Rescue & First Aid
- Field care
- Triage
- Tagging
- Identification of dead
Triage
Triage means to do the most good for the most patients. Four color codes are used:
- Emergent (Immediate) or Priority One (RED)
- Urgent (Delayed) or Priority Two(YELLOW)
- Non-urgent (Minimal) or Priority Three(GREEN)
- Dead (BLACK)
Emergent or Immediate Examples
•Unstable chest/abdomen wounds
•Vascular wounds with limb ischemia
•Incomplete amputations
•Open fractures of long bones
Urgent or Delayed Examples
Stable abdominal wounds
Soft tissue wounds
Vascular injuries with adequate collaterals
Genitourinary tract disruption
Fractures requiring operative intervention
Maxillofacial without airway compromise
Non-urgent or Minimal
These are the walking wounded or those walking “well”. They are directed away from triage area to minimal care area for first aid and non-specialty care. They may be a source of manpower.
Dead / Moribund
These include those whose survival is unlikely even with optimal care. They should be separated from view of other casualties but should not be abandoned. Comfort measures should be provided with minimal staff.
Keys to Successful Field Operations in Disaster Response Scenarios are
- People
- Equipment
- Training
- Organization
Minimum Water Requirements
- Minimum maintenance = 15 liters/person/day
- Feeding centers = 30 liters/inpatient/day
- Health centers and hospitals = 40–60 liters/inpatient/day
- 1 tap stand/250 people not >100m from users
- A large quantity of reasonably safe water is preferable to a small amount of pure water
Minimum Food Requirements
- Minimum maintenance = 2,100Kcals/person/day
- Carbohydrates = 70%
- Proteins = 20%
- Fats = 10%
Minimum Shelter/Space Requirements
- Minimum shelter space = 3.5 m2/person
- Minimum total site area = 45 m2/person for temporary planned or self settled camps
Minimum Sanitation Requirements
- At least 1 toilet for every 20 persons
- Maximum of 1 minute walk from dwelling to toilet (≥6m and ≤50m)
Disposal of Excreta
|
Facility |
Standard |
|
Latrines, family Trench latrines, shallow (for a few days) Trench latrines, (for a few months) |
Not more than four families per latrine without organized, paid maintenance. Latrines should be located at least 6 m from dwellings, 10 m from feeding and health centers, and at least 30 m (and preferably farther) from wells or other drinking-water sources, but no more than 50 m from user. 30 cm wide by 1 m to 1.5 m deep by 3.5 m long per 100 peoples. 70 cm to 100 cm wide by 2 m to 2.75 m deep by 3.75 m long per 100 people |
Mitigation
Activities which actually eliminate or reduce the chance of occurrence or the effects of a disaster. Measures designed to either prevent hazards e.g.
- Protection of vulnerable population and structures
- Improving structural quality of houses, schools, and other public buildings.
- Safety of water supply & sewerage system
Rehabilitation
Actions taken to return to normal or safer conditions. These include:
- Water supply
- Food safety
- Basic Sanitation & Personal Hygiene
- Vaccination
- Nutrition
- Vector Control
Why we are not prepared?
- Traditional approach fail
- Need training
- Need equipment
- Need lots of money
- Fear of unknown
- Misconception ‘It can’t happen here’
- Not interested
- Inherent lethargy
A mnemonic which can help rescuers remember critical information about disaster response and triage:
- D etection
- I ncident command
- S afety and security
- A ssess hazards
- S upport
- T riage and treatment
- E vacuation
- R eallocation and redeployment