Urine routine examination is described under the following headings:
Collection of Sample
Collect early morning, mid-stream urine in a wide neck container and avoid contamination with skin. Label the specimen with patient’s particulars. The sample should be transported to lab as soon as possible. If there is a delay of 1 hour or more, add 0.2 g of boric acid in 20 ml of urine or refrigerate at 4ºC.
Color
Normally urine is clear and pale yellow. In certain abnormal conditions, urine color changes:
- If it is cloudy or turbid, it could be a bacterial infection
- If it is cloudy and red, then either bacterial infection or Schistosomiasis should be suspected.
- If it is brown and cloudy, then black water fever (Plasmodium falciparum) or other conditions that cause intravascular hemolysis should be suspected.
- If it is yellow or orange colored, it may be hepatocellular jaundice.
Smell
Normally it is aromatic. It can be foul smelling in UTI and fruity in diabetes mellitus.
pH and Specific Gravity
Normally specific gravity is 1.004-1.014 and is acidic. Its acidity increases in E. coli infection and is alkaline in Proteus infection.
 Microscopic Examination
Microscopic Examination
Transfer 10 ml of urine in a labeled test tube and centrifuge for 5 minutes. Discard the supernatant and transfer a drop of sediment to slide. Cover it with a cover slip and examine under a microscope. Following features are noted:
1. Bacteria
Only if urine is freshly collected, usually seen as rods but sometimes cocci are found as well
2. White blood cells
They are round, 10-15 micrometer in diameter and contain granules. In urinary infections they appear as clumps. Usually reported as:
- few –up to 10 /HPF
- moderate -11-40 /HPF
- many >40 /HPF
3. Endothelial Cells
Usually seen at 10x. They are seen in vaginal contamination of sample or inflammation of urinary tract. They are reported as few, moderate or many, per low power field. They are nucleated and vary in size and shape.
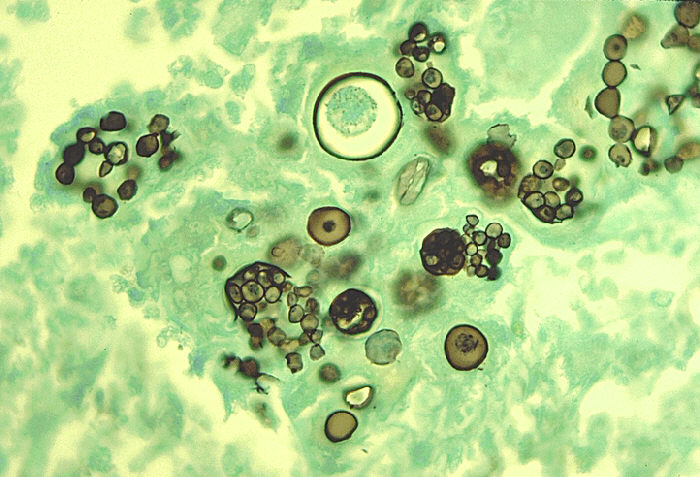
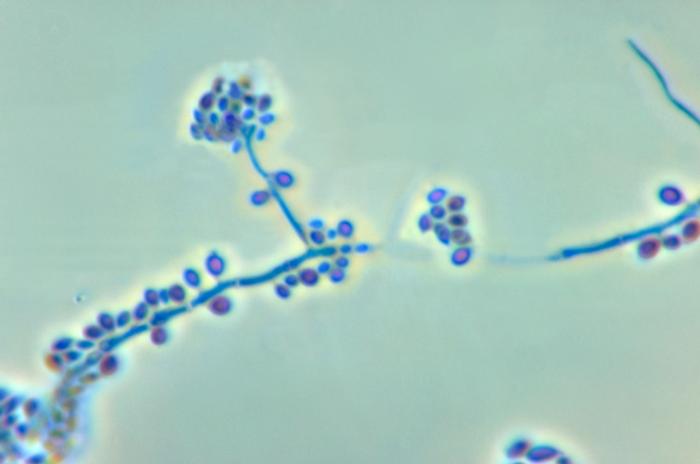
4. Yeast Cells
Differentiated from RBCs by oval shape and budding. Usually seen in women with vaginal candidiasis, diabetics or in immunocompromised.
5. RBCs
Smaller and more refractile and contain no granules. They are seen in Schistosomiasis, heavy bacterial infections, acute glomerulonephritis, calculi or malignancy of urinary tract or sickle cell disease.
6. Casts
They are the solidified proteins, cylindrical in shape because they are formed in tubules, usually seen at low power objective (10x). Following casts may be found in urine:
a. Hyaline Casts –glomerular membrane damage, fever, strenuous exercise
b. Waxy Casts –renal failure
c. Cellular Casts
d. Granular Casts
7. Crystals
They have characteristic refractile appearance. Normal urine contains many chemicals from which crystals may form, therefore, findings of most crystals is insignificant. They should be looked for in fresh urine when calculi or stones are suspected. They may be:
- Cysteine
- Tyrosine
- Cholesterol
- Calcium oxalate
8. Parasites
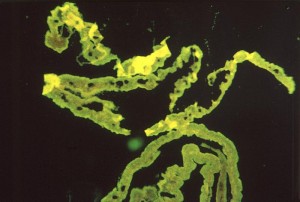
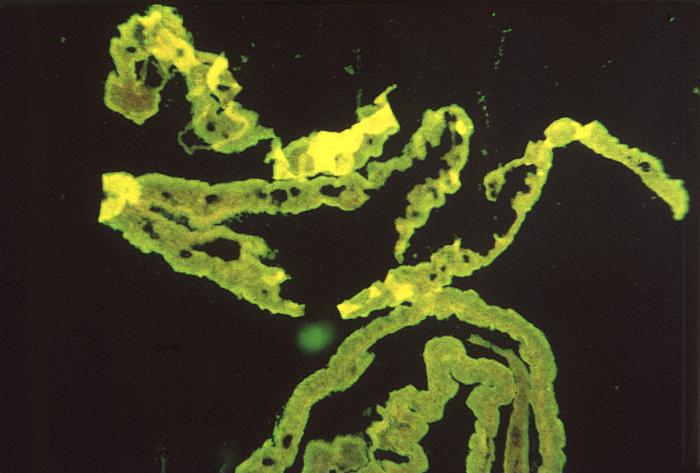
- Trichomonas vaginalis
- Schistosomiasis
9. Biochemical Tests
- Sugars
- Proteins
- Ketone bodies
- Bilirubin
Want a clearer concept, also see
Lecture on Urine Routine Examination
Article on Urine Routine Examination