The diagnosis of edema includes history, physical examination and lab investigations to find out the cause and rule out other important conditions.
History
Site and distribution
Enquiries should be made regarding the site of edema as localized and demarcated sites of edema are usually due to trauma or infection. Oedema may be confined to both lower limbs, for example wit IVC obstruction and pregnancy or affect only a single limb such as the leg with unilateral DVT, or arm following axillary lymph node clearance.
Precipitating factors
Precipitating factors such as trauma and infection may be obvious from the history, and should be excluded. Angio-edema may be precipitated by a known allergen. Lymphedema may result as a complication of infection with filarial nematodes while travelling in endemic areas such as Africa, Asia and Australia. Lymphoedema may also be congenital occurring shortly after birth (Milroy’s disease) or at puberty (lymphedema praecox) or in the third decade (lymphedema trada)
Past medical and drug history
Interruption to lymphatic drainage may result as a complication of irradiation or surgery, especially in the region of the axilla and groin. Obstruction of lymphatic flow can also result from direct involvement of the lymph nodes by lymphoma or secondary to metastatic lymphatic infiltration from tumors. A detailed drug history will identify any offending drug.
Associated symptoms
If there is no obvious precipitating factor in the history, then specific enquiries should be undertaken for each system. Symptoms suggestive of malignancy, in particular should be sought. In addition, it is important to exclude the following conditions:
Cardiac failure
Lethargy, dyspnea, paroxysmal nocturnal ayspnea, cough, ankle edema and abdominal distension from ascities may be some symptoms experienced by patients with cardiac failure
Liver disease
Symptoms of jaundice, pruritus, ankle edema, abdominal distension, haematemesis and confusion (encephalopathy) should be sought to determine the presence of liver disease.
Renal disease -nephrotic syndrome
Severe generalized oedema is the prominent feature with nephrotic syndrome. Patients may also complain of frothy urine due to protenuria
Malabsorption
Wight loss, diarrhoea and steatorrhoea may be some of the features associated with malabsorption
Venous thrombosis
Unilateral leg swelling and pain are the main symptoms of DVT occasionally with iliofemoral vein thrombosis, the entire leg may appear blue (phlegmasia cerulean dolens) or white (phlegmasia alba dolens) bilateral leg edema with the onset of dilated superficial collateral veins on the trunk and abdomen is suggestive of IVC obstruction.
Examination
Inspection
Assessment of the distribution of edema may narrow the differential diagnosis. Generalized causes tend to present with dependent edema, with fluid accumulating in the ankles in ambulant patients with the sacrum in recumbent patients
Cardiovascular system
With cardiac failure, palation of the pulse may reveal tachycardia with pulsus alternans. The measured blood pressure may be low due to systolic failure. The JVP is elevated and a third heart sound with bilateral coarse pulmonary crepitations may be auscultated. Hepatomegaly due to liver congestion and ascites may also be present.
Abdominal examination
Generalized wasting from malabsorption or malignancy may be appreciated on inspection. Clubbing, palmar erythema, Dupuytren’s contracture, jaundice, spider naevi and gynaecomastia are signs of liver disease. Dilated collateral veins on the abdomen may be due to portal hypertension or IVC obstruction; therefore determine the direction of blood flow. Below the umbilicus the direction of blood flow is inferior with portal hypertension, and superior with IVC obstruction. Organomegaly due to carcinoma may be present and predispose to venous thrombosis. Pelvic malignancy may also result in venous outflow obstruction.
Legs
The legs are examined for the presence of tenderness and swelling Circumferences of both the thighs and calves are compared. Marked painful erythematous unilateral swelling may be indicative of DVT.
General investigations
Urinalysis
Heavy proteinuria with nephrotic syndrome
Free blood count (FBC)
WBC elevated infection, Hb decreased, Malabsorption and DVT
U&Es
Urea and creatinine elevated with renal failure
LFTs
Abnormal in liver disease
Serum albumin
Reduced with nephrotic syndrome, liver disease, malabsorption and malnutrition
Specific investigations
24 hour urine collection
>3.5 g of protein with nephrotic syndrome
Renal biopsy
To determine the cause of nephrotic syndrome in adults
Echocardiography
Ventricular dilatation and impaired function with cardiac failure
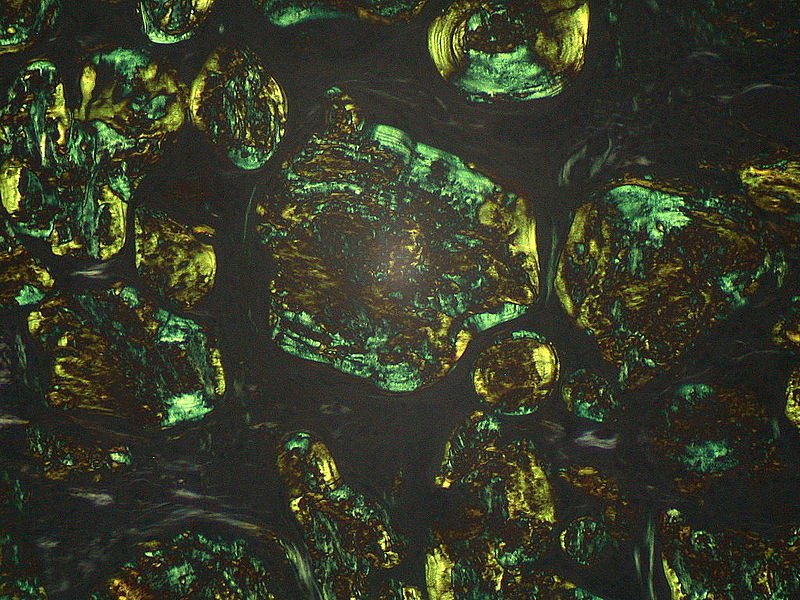
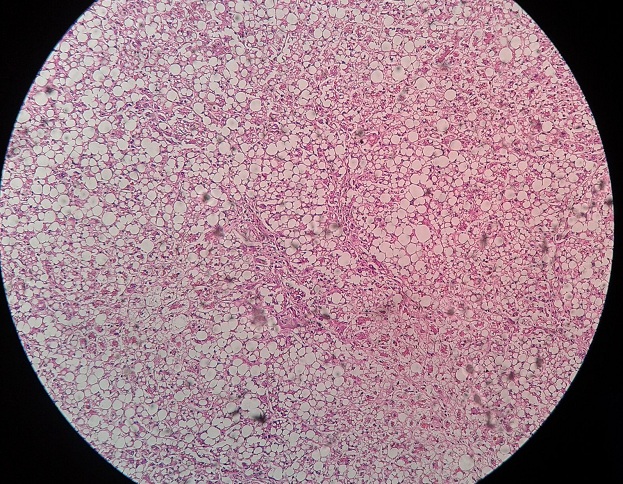
Liver biopsy
Liver cirrhosis
Faecal fat estimation
Malabsorption
Duplex Doppler deep veins of the leg
DVT of the leg
Venography
Below-knee DVT, IVC obstruction
Lymphangcography
Lymphatic obstruction of any cause
Pelvic ultrasound or CT
Pelvic tumours