The investigation of an individual with possible hyperlipidemia or one shown to be hyperlipidemic on a fasting sample on at least one previous occasion requires both clinical assessment and laboratory testing
Clinical assessment
This involves taking a good history and conducting a full physical examination during the patient’s first clinic visit.
History
The patient should be questioned about the following aspects of his own personal history:
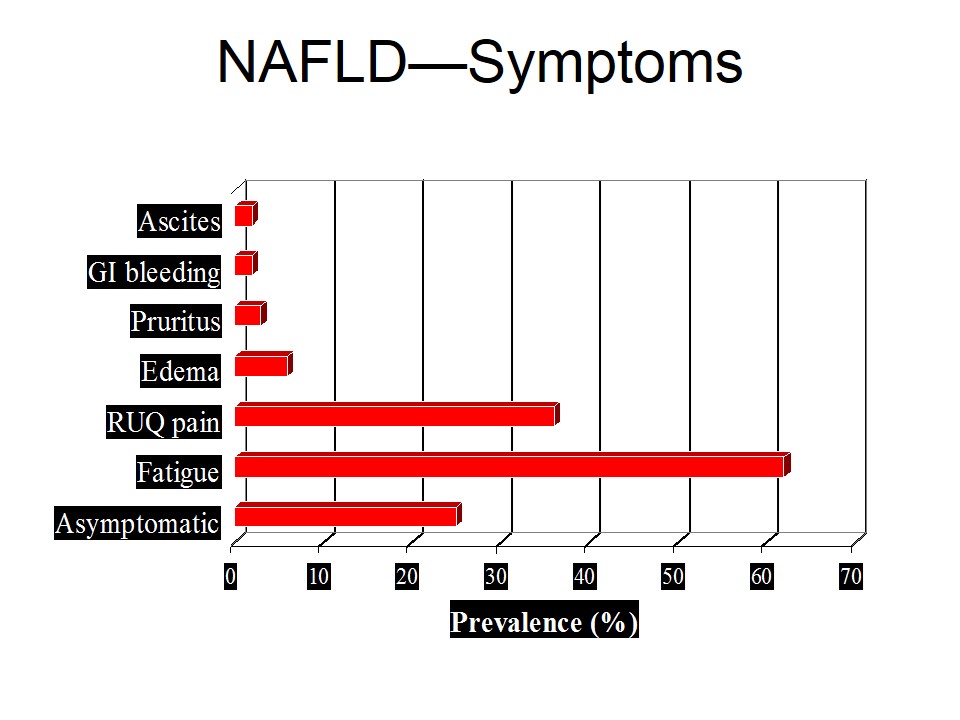
- Symptoms of vascular insufficiency such as angina
- Results of any previous plasma lipid investigations.
- Any previous complications, e.g. coronary artery bypass graft, angioplasty, cholecystectomy for gall stones.
- Dietary habits,
- Lifestyle habits, such as smoking, exercise, drugs taken currently.
- Any intercurrent disease such as diabetes, thyroid dysfunction, renal disease.
Family History should also be carefully recorded. This includes eliciting details of:
- Premature coronary heart disease (CHD) in immediate relatives, age of onset and death due to CHD.
- History of hyperlipidemia in family members
- Presence of other risk factors for CHD, such as hypertension, diabetes.
Clinical examination
Blood pressure measurements to exclude (or document) hypertension, and a search for external signs of hyperlipidemia (corneal arcus, eruptive / tendonous xanthomata, xanthelesma) are particularly relevant in such patients.
Investigations
The first and most important concern is to confirm the presence of hyperlipidemia in a sample taken after an overnight fast of at least 10- hours duration.
The initial testing should include lipid profile measurements of
- Total cholesterol
- Triglyceride
- HDL cholesterol which enables calculation of LDL cholesterol.
Other tests, if indicated, can be performed after the results of the initial tests are available for interpretation.
Laboratory Investigations
1. Serum total cholesterol and triglycerides
Measurement of plasma or serum total cholesterol and triglycerides were traditionally used for the assessment of hyperlipidemia and its attendant risks of CAD.
2. Plasma HDL and LDL Estimation
Calculation of LDL-c (Friedewald Formula)
When the plasma triglyceride concentration is >4.5 mmol/L, the formula is invalid
LDL-c=total cholesterol – HDL-c – (triglyceride/2.2)
(Note: all three measured parameters in mmol/L)
If a non-fasting specimen is used, the VLDL triglyceride value may be inaccurate and LDL cholesterol is underestimated.
3. Additional Biochemical Markers these include
Serum Electrophoresis
● Serum apoliproteins (apo A-I, apo –B)
● Lp (a)
● Subfractions of HDL
Genetic sequencing
● Apo E phenotypes or genotypes.
Phenotyping or genotyping of apolipoprotein E
Phenotyping can be carried out using iso-electricfocusing gel electrophoresis;
The genotyping assay uses molecular genetics techniques.
They tests have specific application and provide useful information in selective cases, e.g. Alzheimer’s disease.
Sample Collection for Lipid Analysis:
Requirements and pitfalls:
Both plasma and serum may be used for most of the lipid analysis.
Special Precautions in the patient preparation and specimen collection. To obtain reliable results, it is important to ensure that the patient.
- Fast in for 10-14 hours prior to blood sampling.
- Not be severely stressed before or during the blood sampling.
- Reports any current use of medication.
A Fasting Specimen is essential for triglyceride analysis because plasma triglyceride concentration increase as soon as two hours postprandially (after ingestion of a meal containing fats) and reach a maximum at 4-6 hours post – meal.
For the same reason, non fasting samplings are also not suitable for the determination of serum LDL estimations using the Friedewald calculation.
Hyperchylomicronemia causes incomplete precipitation of the apo B- containing lipoproteins, leading to falsely elevated HDL-c values in blood samples.
Unlike triglycerides, plasma cholesterol levels do not rise acutely after a fatty meal.
Severe metabolic traumas such as a myocardial infarct adversely affect serum lipid levels. Plasma cholesterol results after an MI can be very misleading often falling markedly due to the trauma. It normally takes 3-6 weeks for the cholesterol levels to return to pre infarct levels.
Stress also causes mobilization of free fatty acids and results in artefactually elevated plasma triglyceride levels.